Achilles Tendinopathy
What is it?

Achilles tendinopathy is an overuse injury that involves dysfunction and local tendon pain with excessive loading (Malliaras et al., 2013). The tendon structure can be altered resulting in a tendon that is less capable of sustaining repeated load. An injury to the Achilles Tendon can severely impact a patient’s daily activities as it is one of the major locomotor tendons in the body (Malliaras, Barton, Reeves, & Langberg, 2013).
Change in the name
Previously, tendon pain was given the term ‘tendinitis’. The suffix ‘itis’ implies that the tendon is ‘inflamed’. Over time our understanding of tendon pathology has changed and new research has shown that it is not necessarily an inflammatory process, but rather the breakdown of the matrix of the tendon and the accumulation of our ‘failed healing response’ that causes the pain.

Physiotherapy role
Physiotherapy is crucial in the management of Achilles tendinopathy as the treatment will go beyond just reducing the symptoms temporarily. The rehabilitation program will address the underlying cause of the pathology by conditioning the tendon to become more resilient to load for the future.

Treatment can broadly be divided into pain management and rehabilitation stages. Reducing pain irritability is often an initial priority with load management; isometric exercise and adjunct therapies being quite useful in this stage.
When Achilles tendon pain stabilises, the tendon is then further loaded with more function-specific, energy storage and sports-specific exercise. Progression is based on a pain and strength criteria to enable return to full function (whether it be every day activities or a specific sport).
Continuum of tendon pathology
Tendinopathy has been described as a continuum of pathology that has three distinct stages. It is described with distinct stages for convenience, however being a continuum, there is continuity between stages (J. Cook & Purdam, 2009).
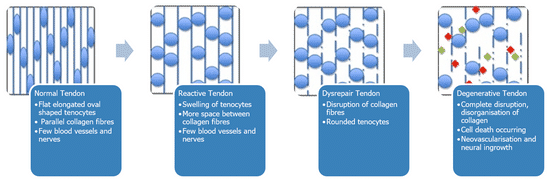
1) Reactive Stage
This stage is characterised by a sudden increase in load or impact to the tendon. The tendon cells will absorb more water content and get swollen. If the load is reduced and time is given for the tendon to adapt, it will return to normal. If excessive load continues, it will progress to the next stage.
2) Disrepair Stage
This stage occurs when the tendon fails to heal itself. The collagen fibres become disorganised and new blood vessels/ nerves will grow in the tendon to try to promote healing. With appropriate management and load modification it is still possible to return this tendon to normal.
3) Degenerative Stage
Chronic overload of tendons will eventually create an environment of tendon breakdown. This is the main characteristic of the degenerative stage. Small lesions will develop where the tendon cells and collagen have broken down. Although these lesions are irreparable, we often use the analogy of a doughnut – even though the doughnut has a hole in its centre, it doesn’t matter because the rest of the doughnut around the hole is still functioning tissue that can be loaded.
Patients need to be aware that
Pain is poorly correlated with imaging pathology and not necessarily equal to harm
Pain during rehabilitation is acceptable and expected
Before loading commences, an accurate diagnosis must be made to determine which stage of pathology the patient is in
Typical loading program
| Stage 1 | * isometric exercises that isolate the affected muscle-tendon unit *holds of 30–60 seconds 3-4 reps x 4/per day * effective in reducing pain and commencing load of the myotendinous unit e.g. seated calf raises with weight on lap. |
| Stage 2a | *isotonic loading in limited range *commenced when minimal pain during isometric loading (Isotonic load is important to restore muscle bulk through range of movement whilst avoiding compressive positions) e.g. calf raises with reduced range. |
| Stage 2b | *isotonic load into full range (The goal is to improve tendon load tolerance in ranges that are relevant to the patient’s functional goals and may involve some compression) e.g. calf raises on a step |
| Stage 3 | *energy storage and power loading exercises * for patients who need to participate in explosive movements e.g. jogging on the spot or hopping |
| Stage 4 | *return to sport or functional daily tasks *gradual and can be commenced when the tendon is tolerant to energy storage progressions that replicate functional demands of the individual’s sport or activity |
Have a chat with our team today and start your recovery journey.
Sports Med. 2013 Apr;43(4):267-86. doi: 10.1007/s40279-013-0019-z. Achilles and patellar tendinopathy loading programmes : a systematic review comparing clinical outcomes and identifying potential mechanisms for effectiveness.
Sorry, comments are closed for this post.