Vertigo
What is vertigo?
Vertigo is an abnormal sensation of motion; Disequilibrium is a sensation of impending fall or of the need to obtain external assistance for proper locomotion. Positional vertigo or Benign paroxysmal positional vertigo (BPPV) is the most common. It is the sensation of spinning that occurs after the patient’s head has moved to a new position. This is with respect to gravity and in most cases of inner ear origin.

Vertigo and disequilibrium are common symptoms in a primary care practice. Since these symptoms can be associated with serious disease, it is important to evaluate them properly. Any disorder that interferes with the sensory function of vision, balance, or proprioception or that affects the oculomotor control system can result in disequilibrium or vertigo. The history centres on establishing the underlying disease in these sensory systems or in the central mechanisms that mediate responses to these sensory systems. (Horst R. Konrad, 1990)
Differential Diagnoses of Vertigo
– Cervicogenic dizziness
– Viral or bacterial labyrinthitis
– Ménière’s disease
– Vestibular Neuritis
Cervicogenic Dizziness
Cervicogenic dizziness (CGD) is a clinical syndrome characterized by the presence of imbalance, unsteadiness, disorientation, neck pain, limited cervical range of motion (ROM), and may be accompanied by a headache. There are no definitive clinical or laboratory tests for CGD and therefore CGD is a diagnosis of exclusion. Cervical arterial dysfunction (CAD) and whiplash associated disorder (WAD) are non-vestibular pathologies that can mimic CGD and must be ruled out in the examination.
Dix-Hallpike technique (DHT), can then be used to determine if the vestibular system is causing the dizziness. Once vestibular pathologies have been ruled out, the clinician should examine the cervical spine, followed by the cervical neck torsion test and cervical relocation test to help confirm or exclude the diagnosis of CGD. (Reiley, 2017).
LATEST RESEARCH
A 2019 double-blind randomised controlled trial by Monreno et al wanted to test the effectiveness of the Epleys manoeuvre for posterior canal BPPV. The intervention group showed better results in the unadjusted analyses at 1 week, with a lower rate of positive DHT with nystagmus. A positive baseline DHT with nystagmus was associated with a reduction in vertigo severity and better positive DHT rates in the intervention group in the multivariate analyses. They concluded that, a single Epley’s manoeuvre performed in primary care is an effective treatment for reversing a positive DHT and reducing vertigo severity in patients with baseline nystagmus in the DHT.
Treatment and Rehabilitation
Neck massages alone rarely work in resolving dizziness with the neck pain. However it can be used as an adjunct, due to the secondary nature of guarding and muscle tension associated with dizziness that most patients experience. Several studies have reported that approximately 75 percent of patients improve with conservative treatment of the neck such as gentle mobilizations, exercises, and instruction in proper posture and neck positioning (Wrisley).
Vestibular training exercises such as self-administered repositioning manoeuvres, gaze stabilization exercises, falls prevention training, and patient education are shown to be beneficial in reducing the symptoms of BPPV and improve quality of life (Bhattacharyya, 2008).
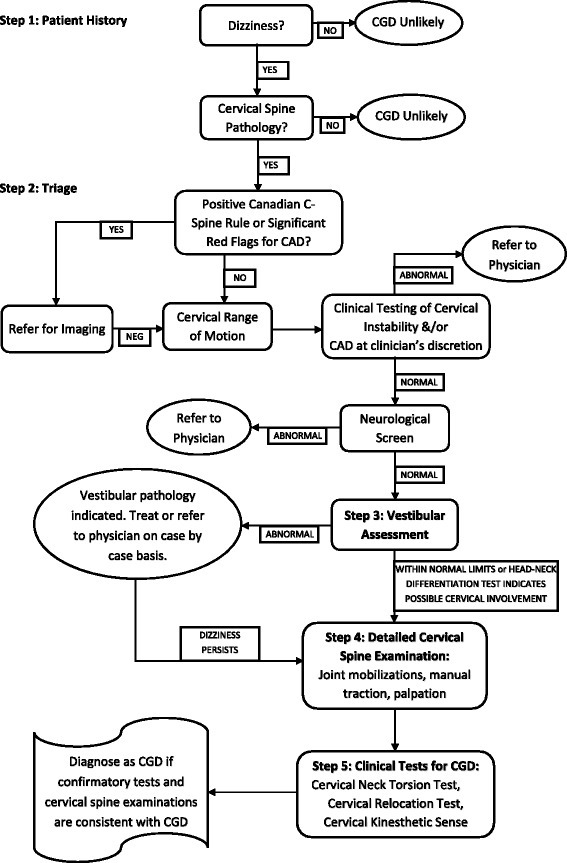
Flowchart for Cervicogenic Dizziness diagnosis
PHYSIOTHERAPY TREATMENT
After a very thorough screening assessment in clinic :
ACUTE
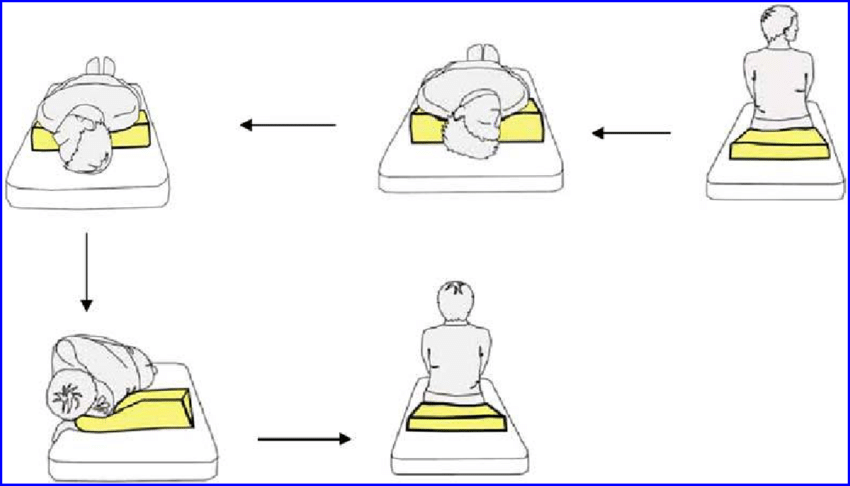
- Administering Epley’s and Dix-Hallpike manoeuvre in clinic
- Gentle facet joint mobilisation in non-irritable position as able
- Cervical neck muscle stretches
- Postural correction exercises
- Early stages vestibular retraining exercises
SUB-ACUTE
- Cervical/Thoracic Spine strengthening
- High level vestibular training exercises
- functional retraining
- return to sport/exercise
- Workstation ergonomic (if required)
At Mediphysio our physios are all trained in the screening of cervical conditions and will be able to assist you what is the best management pathway for your dizziness, whether that be physiotherapy treatment or a referral back to a specialist healthcare provider and potentially scans. Give us a call today or book in your appointment online.
References:
- Horst R. Konrad. – Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition.
- Reiley, 2017 – How to diagnose cervicogenic dizziness
- Monreno et al 2019 Effectiveness of the Epley manoeuvre in posterior canal benign paroxysmal positional vertigo: a randomised clinical trial in primary care
- Wrisley – https://vestibular.org/article/diagnosis-treatment/types-of-vestibular-disorders/cervicogenic-dizziness/
- Bhattacharyya, 2008 – https://www.physio-pedia.com/Benign_Positional_Paroxysmal_Vertigo_(BPPV)#cite_note-Bhattacharyya2-23
Sorry, comments are closed for this post.