Adhesive Capsulitis the “Frozen Shoulder”

What is a frozen shoulder?
A frozen shoulder (ADHESIVE CAPSULITIS) is a common condition affecting 3% of the population. It usually affects people over the age of 40 years and is more common in women than in men.
It is a primary idiopathic condition where the inflammatory pathological process of excessive scar tissue (arthrofibrosis) is formed across the glenohumeral joint ( shoulder joint) leading to stiffness, pain and dysfunction of the shoulder. (Le et al ., 2017). It may be triggered by an injury or previous surgery (heart or breast) but it is also associated with a range of medical conditions including diabetes, thyroid disease, Parkinson’s disease and inflammatory disorders. It is characterized by an initially painful and later progressively restricted active and passive glenohumeral (GH) joint range of motion with spontaneous complete or nearly-complete recovery over a varied period of time
Clinical diagnosis is often difficult and not caught early as it is made on the basis of medical history and physical exam and is often a diagnosis of exclusion.
How do patients present with the condition Adhesive Capsulitis?
Patients presenting with adhesive capsulitis will often report an insidious onset with a progressive increase in pain, and a gradual decrease in active and passive range of motion. External rotation is often the first motion affected on clinical examination, with steady global loss of ROM with disease progression(Le et al ., 2017).
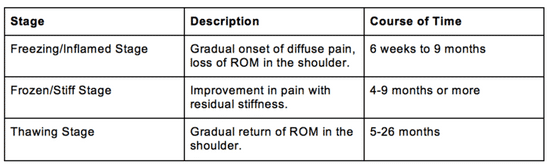
The frozen shoulder phases
This condition is characterised by specific phases stated below which overlap. Overall though, frozen shoulder is a self-limiting condition which may take up to up to two years to resolve.
Adhesive Capsulitis Treatment
Rymaruk and Peach, 2017., reported a statistically significant benefit with the addition of physiotherapy after a glenohumeral joint steroid injection vs injection alone.
As we are still trying to find the true causation of adhesive capsulitis, the body of literature shows varying front line treatment modalities in the forms of steroid injections, hydro-dilation of the capsule or surgical capsular release to reduce pain and disability scores. All modalities show varying improvements and no one treatment seems to statistically show one better outcome than the other. This is due to adhesive capsulitis being a multifactorial condition.
What all studies do show as mentioned previously by Rymaruk and Peach, 2017., is that a combined front line modality, in conjunction with physiotherapy in providing a exercise based rehab program, gives the patient the best outcome measures in pain, disability and function.
Physio management of frozen shoulder
The most important aspect of the treatment is to understand that this is a condition that should get better by itself. The mainstay of treatment is to use the shoulder as much as possible (within the limits of your discomfort). It is important to avoid immobilising the arm or stop using it as this will cause the condition to deteriorate.
- Freezing Phase:
- pain relief/management is the primary goal in this stage i.e. heat, TENS, dry needling, soft tissue massage, gentle ROM
- advice and education for prevention of further loss in global range of motion of shoulder joint through gentle ROM
- Frozen Phase:
- encouraging ADLs within functional limits
- safe exercise program->not aggressive
- maintaining current range in all directions of shoulder and other upper limb joints
- Thawing Phase:
- exercise progressions, strengthening exercises to control and maintain increased range of movement. Physiotherapy is most effective during this thawing phase.

Medical management options
A study by Dennis et al, looked at the practice of health professionals (general practitioners, physiotherapists and orthopaedic surgeons) in managing idiopathic frozen shoulder in the painful (freezing) as well as resolution (thawing) phase. Conservative treatment in the form of watchful waiting, patient education, oral pain killers and steroids as well as physical therapy emerged as the most commonly used interventions for patients in the early painful phase. 47% of respondents recommended surgery for patients in the resolution phase, with 24.1% recommending arthroscopic capsular release, 21% manipulation under anaesthesia and 2% open capsular release. 19.4% recommended physical therapy, 5.1% arthrographic distension, 2.6% injections and 12.4% conservative treatment for the resolution phase.
So what now?
There still remains conflicting data as to which medical treatment method is best for patient outcomes. However, the volume of research and studies on adhesive capsulitis assists us as medical practitioners cipher the least effective options to assist in best patient outcomes. We treat each case individually and decide which factors are most at play and adapt each program case by case.
To find out more about frozen shoulder speak to one of our team members today or BOOK NOW a shoulder review.

References:
Yang et all., 2020 https://europepmc.org/article/med/32032093
le et al 2017 – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5384535/
Rymaruk et al., 2017 –
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5706054/ Image credit / graph https://www.doldmd.com/adhesive-capsulitis-frozen-shoulder
Sorry, comments are closed for this post.